まず我が国に未導入のdeviceに関しては(Table 1:網掛け部分),2012年に「先天性心疾患に対するカテーテル治療 ~本邦への導入が期待されるdevice~」と題したReviewが日本小児循環器学会雑誌に掲載された1).すでに4年もの歳月が経過したが,取り上げられた10のdevicesのうち実際に導入されたものはNykanen RF Puncture Wire(Baylis Medical, Canada)(2014年),およびFigulla® Flex II ASD devices(Occlutech GmbH, Jena, Germany)(2016年)の2つに過ぎない.残る8つのdevices: GORE® HELEX® Septal Occluder(現:GORE® CARDIOFORM Septal Occluder)(W.L. Gore & Associates, Inc. USA),Amplatzer® Duct Occluder(ADO)IIおよびII AS(Additional Sizes)(St. Jude Medical Co. USA),Amplatzer® Muscular VSD Occluder(St. Jude Medical Co. USA),Covered Cheatham-Platinum(CP)Stent™(NuMED Inc. USA),Advanta® V12 Covered Stent(Atrium Medical Inc. USA),Melody® Transcatheter Pulmonary Valve(Medtronic Heart Valve Inc. USA),Edwards SAPIEN XT® Transcatheter Heart Valve(Edwards Lifesciences Co. USA)がいまだ導入されていない(ただしCP Stent™に関しては医師主導治験が進行中).
Table 1 Devices used for catheter intervention in congenital heart diseases.| Device | CE (EU) | FDA (USA) | Japan |
|---|
| Occluder | ASD | Amplatzer® Septal Occluder | 1998 | 2001 | 2005 |
| Occlutech® Figulla® Flex II ASD device | 2012 | Unapproved | 2016 |
| GORE® CARDIOFORM Septal Occluder | 2011 | 2006 | Unapproved |
| PFO | Amplatzer® PFO Occluder | 1998–2007 | Unapproved | Unapproved |
| Occluthch® Figulla® Flex II PFO device | 2012 | Unapproved | Unapproved |
| PDA | Amplatzer® Duct Occluder | 1998 | 2003 | 2008 |
| Amplatzer® Duct Occluder II/II AS | 2008 | 2014 (AS: Unapproved) | Unapproved |
| Occluthch® PDA Occluder | 2012 | Unapproved | Unapproved |
| vessel | Amplatzer® Vascular Plug | 2004 | 2003 | 2012 (except for heart and intracranial vessels) |
| Amplatzer® Vascular Plug II | 2007 | 2007 | 2013 (except for heart and intracranial vessels) |
| Amplatzer® Vascular Plug III | 2008 | Unapproved | Unapproved |
| Amplatzer® Vascular Plug 4 | 2009 | 2012 | 2014 (except for heart and intracranial vessels) |
| VSD | Amplatzer® Muscular VSD Occluder | 1998 | 2007 | Unapproved |
| Amplatzer® Membranous VSD Occluder | 2006 | Unapproved | Unapproved |
| Stent | PALMAZ® Medium stent | 1998 (peripheral vessel,biliary duct)* | 1991 (iliac artery)* | 1996 (peripheral vessel) |
| 2002 (renal artery)* |
| PALMAZ® Large stent | 1998 (iliac artery)* | 1991 (iliac artery)* | 1996 (peripheral vessel) |
| PALMAZ® EX Large stent | 1998 (peripheral/great vessel, biliary duct) | 1999 (biliary duct) | 2004 (biliary duct) |
| PALMAZ® GENESIS® Medium stent | 2001 (peripheral vessel/biliary duct) | 2001 (biliary duct) | 2004 (renal artery) |
| PALMAZ® GENESIS® Large/EX Large stent | 2001 (peripheral vessel, biliary duct) | 2001 (biliary duct) | Unapproved |
| Express™ Vascular SD stent | 2003 (peripheral vessel) | 2008 (renal artery) | 2010 (renal artery) |
| Express™ Vascular LD stent | 2002 (peripheral vessel) | 2010 (iliac artery) | 2007 (iliac artery) |
| Omunilink Elite® Peripheral stent system | 2009 (biliary tree, atherosclerotic lesions) | 2012 (iliac artery) | 2014 (iliac artery) |
| Cheatham-Platinum Stent™ | 2004 | 2016 | Unapproved (under clinical trial) |
| Covered Cheatham-Platinum Stent™ | 2004 | 2016 | Unapproved |
| Valve | Melody® Transcatheter Pulmonary Valve | 2006 | 2010 | Unapproved |
| Edwards SAPIEN XT® Transcatheter Heart Valve | 2007 | 2016 | Unapproved |
* PALMAZ® Medium/Large stent: handling end in EU and USA, Hatching: Unapproved in Japan
AS: additional size, ASD: atrial septal defect. PDA: patent ductus arteriosus, PFO: patent foramen ovale, VSD: ventricular septal defect |
さらに,導入されたdeviceの承認年度を見ると,CE, FDAの承認と日本での承認にはいずれも5~10年のtime lagがある(Table 1).いかに本邦への導入に時間を要するかが明らかである.
続いて主要疾患におけるカテーテル治療の選択肢と,それに適したdeviceが日本で入手可能か,適応を取得しているかについて検討する.
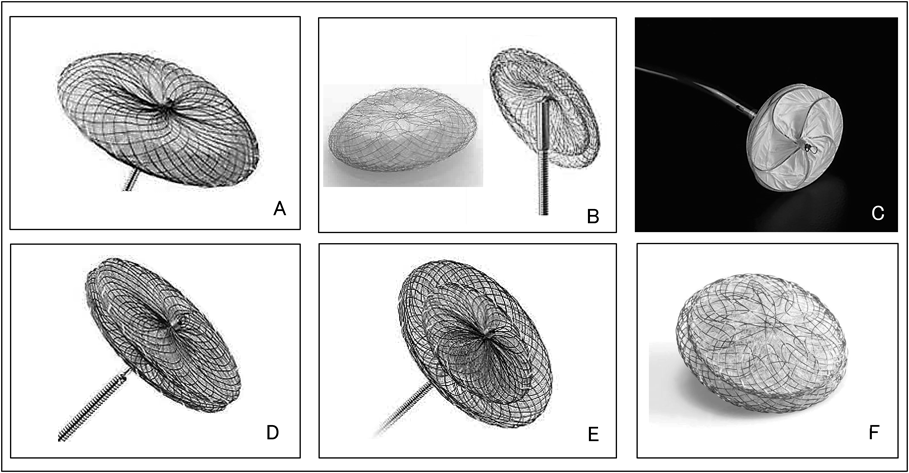
まず心房中隔二次孔欠損の閉鎖では,2005年にAmplatzer® Septal Occluder(ASO)(St. Jude Medical Co. USA)(Fig. 1-A)が,2016年にOcclutech® Figulla® Flex II ASD device(Fig. 1-B)が導入され,第一選択治療法の地位を確立している.国内未導入のGORE® CARDIOFORM Septal Occluder(Fig. 1-C)は前2者と異なりself-centeringではなく,device径は欠損孔径の2倍以上が推奨されていることから,閉鎖できる欠損孔の大きさは通常17 mm以下という限界がある.しかしその形態および柔軟な材質のため心侵食のリスクが低く2),この点において導入に一考の価値はある.多孔性欠損に対してはAmplatzer® cribriform septal occluder(St. Jude Medical Co. USA)(Fig. 1-D)が用いられ,国内でも認可されている.
卵円孔に関しては,Amplatzer® PFO Occluder(St. Jude Medical Co. USA)(Fig. 1-E),Occlutech® Figulla® Flex II PFO device(Occlutech GmbH, Jena, Germany)(Fig. 1-F)が専用の閉鎖deviceである.卵円孔閉鎖の主目的は脳梗塞の再発抑制および偏頭痛の抑制であるが,deviceによる閉鎖と従来の薬物療法のいずれが優れているか,いまだ一定の見解に達していないことから3, 4)FDAでは認可されておらず,国内にも導入されていない.
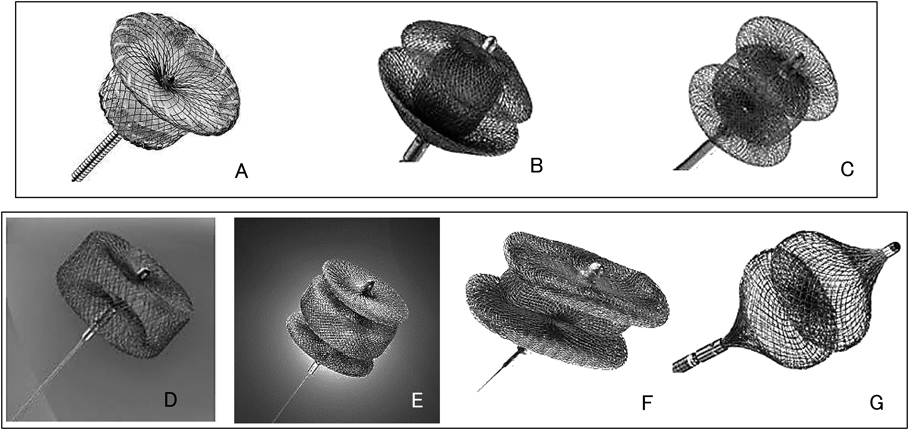
動脈管に関してはAmplatzer® Duct Occluder(ADO)(St. Jude Medical Co. USA)(Fig. 2-A)の登場により,coilでは閉鎖が困難な症例にもカテーテル治療の可能性が広がり,かつ短時間で安全に閉鎖できるようになった.わが国でも2008年の承認以来,中心的治療法になっている.ただしADOの適応は,合併症の面から体重6 kg以上の症例とされている.ADO IIおよびII AS(Fig. 2-B, C)は,より細いワイヤーを用い,かつポリエステル膜を除くことでより細いデリバリーシースに適合し,さらに肺動脈側,大動脈側の双方にretention discを装着したことで,肺動脈側,大動脈側のいずれからも留置できるように改良されており,体格の小さい症例へ治療域が拡大した5, 6).また体格の小さい症例や特殊な形態の動脈管に対してはAmplatzer® Vascular Plug(AVP),AVPII, AVP4(St. Jude Medical Co. USA)(Fig. 2-D, E, G)やASO,Amplatzer® Muscular VSD occluder(Fig. 3-B)を用いることの有用性も報告されているが7–10),ADO II/II AS, Amplatzer® Muscular VSD occluderは未導入,AVP family, ASOはoff-label useである.
血管の閉塞に関しては近年相次いでAVP family(Fig. 2-D–G)が国内に導入されたことにより(IIIを除く)治療の幅が広がった.かつmicro coilの種類が豊富であり,側副血行路の閉塞に関しては選択の幅が広い.冠動脈瘻はcoilでの閉塞が困難な場合,AVPやADOでの閉鎖が考慮されるが10, 11),冠動脈瘻は心臓に関連する血管との見解からAVP familyの適応外とみなされ,AVP, ADOともoff-label useとなる.
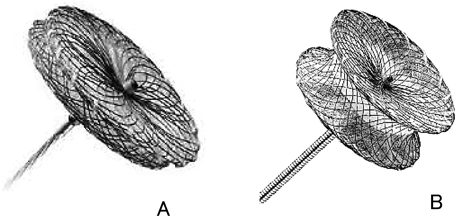
心室中隔欠損では,傍膜様部欠損に対してAmplatzer® Membranous VSD Occluder(St. Jude Medical Co. USA)(Fig. 3-A)が開発されたが,房室ブロック,房室弁逆流等の合併症が8.6%に見られ12)FDAおよび国内では認可されていない.現在,改良型のAmplatzer® Membranous VSD Occluder 2(St. Jude Medical Co. USA)での検討が行われている13).筋性部欠損では,外科的閉鎖が困難な症例の閉鎖にAmplatzer® Muscular VSD Occluder(Fig. 3-B)が用いられる14).AHAによるScientific Statementでは,体重5 kg以上の例でのカテーテル治療の推奨レベルはクラスIIa,体重5 kg未満の例でのhybrid治療はクラスIIaとなっているが15),国内には導入されていない.
Fontan循環のFenestrationに関しては,バルーン閉鎖試験で十分に血行動態が維持できる場合,カテーテルによる閉鎖術の推奨レベルはクラスIIaとなっている15).deviceに関しては各種ASD occluders, PFO occluders, VSD occluders, embolization coils, vascular plugs, covered stentsが挙げられている.Side by sideに作成したhole状のfenestrationにはASD occludersが16),Goretex graftを用いた筒状のfenestrationにはvascular plugsの有用性がうたわれている17)が,国内ではいずれもoff-label useとなる.
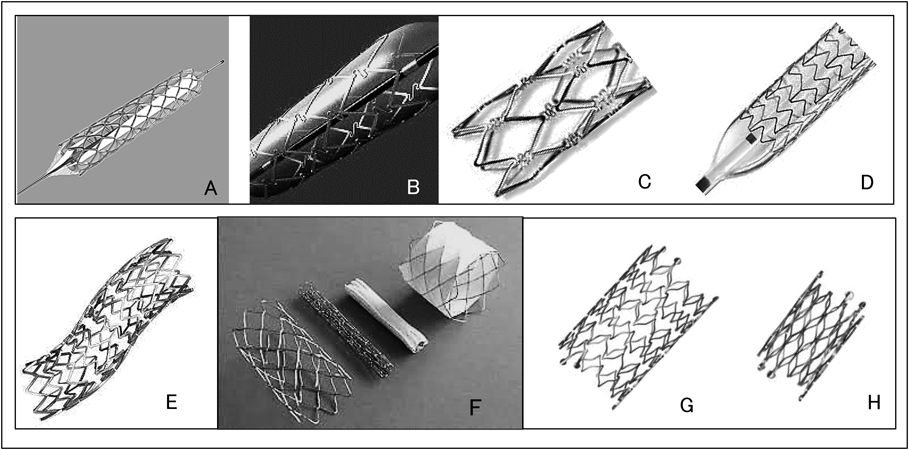
血管形成術においては,バルーン形成術の効果が十分でない場合,stent留置が考えられる.小児では必然的に体格の成長という問題が付随するため,stent留置はすべての血管において成人相当サイズのstentが留置可能な場合,もしくは将来そのサイズにまで拡大可能な場合が適応とされている15).わが国では特に大径のstentの選択肢が少ないこと,我々の領域で主に対象となる肺動脈,肺静脈,大動脈,大静脈,動脈管にはいずれのstentも適応がないことが問題となる(2016年5月末現在).PALMAZ® seriesでは,PALMAZ® stent(Cordis Corporation, USA)(Fig. 4-A)の直線型のステントデザインにS型形状を追加したPALMAZ® GENESIS® stent(Cordis Corporation, USA)(Fig. 4-B)が登場した.柔軟性が高く病変部への到達が容易なこと,よりlow profile化され血管合併症が低減したことにより,EU, USAではすでにPALMAZ® Medium/Large stentの供給は終了し,PALMAZ® GENESIS® stentに置き換わっている.また316Lステンレス鋼を用いていたPALMAZ® stentおよびPALMAZ® GENESIS® stentに対し,L605 cobalt chromiumを用いることでより放射線不透過性が増し,low profile化されたPALMAZ® BLUE® stent(Cordis Corporation, USA)(Fig. 4-C)も市場化されている.国内にはPALMAZ® GENESIS® Large/Extra Large stentおよびPALMAZ® BLUE® stentが未導入である.
大動脈縮窄の治療においては,治療部位の動脈瘤形成,解離のリスクはバルーン血管形成術に比較し,stent留置のほうが低いと言われている15).CP Stent™(Fig. 4-F)はplatinum iridium合金ワイヤーを“zig”型に形成し24K金を用いてレーザー接合したstentで,径12~24 mmに拡大可能である.従来のstentに比較して硬度を増しradial方向の強度を高くしたことで,成人の術後再狭窄などに適している.Covered CP Stent™はCP Stent™を伸長可能な筒状のePTFE(expanded polytetrafluoroethylene)でカバーしたstentである.USAにおけるCP Stent™留置の多施設臨床試験:COAST(Coarctation of the Aorta Stent Trial)で,通常のバルーン血管形成術に比較して良好な成績が報告された18).この試験に続いて①内腔3 mm未満の重症縮窄,マルファン症候群,ターナー症候群を含む結合組織異常,60歳以上(バルーン血管形成術やstent留置ではリスクが高いと考えられる例),②外科治療やカテーテル治療に合併した大動脈壁損傷例(COAST登録例を含む)を対象にCovered CP Stent™を用いた多施設臨床試験が行われ(COAST II),すでに短期の有用性は報告されている19).大動脈壁損傷に関しては術後遠隔期のみならず,カテーテル治療中に発生した瘤,解離の緊急治療としてもこのCovered Stent留置を考慮すべきとされている19, 20).
また経皮的バルーン肺動脈弁形成術,右室流出路stent留置術,後述する経皮的肺動脈弁留置術において,特に術後で高度石灰化が見られる例では治療中の破裂のリスクが有意に高いため,緊急的回避手段としてCovered Stentを備えておくよう推奨されている15, 21, 22).CP Stent™に関しては国内での治験が進行している(2016年5月末現在).USAと同様に先天性心疾患に適応のある初のstent導入となる見込みである.
肺静脈狭窄では,バルーン血管形成術,stent留置術などが試みられるが,周知のとおり成績は決して良好とは言えない.このため内膜増殖による狭窄を抑制する目的でdrug eluting stent(DES)留置が試みられ,有用例の報告も見られる23).国内ではCYPHER™ DES(シロリムス)(Cordis Corporation, USA),TAXUS® DES(パクリタキセル)(Boston Scientific, USA),XIENCE™ DES(エベロリムス)(Abbott Vascular, USA),Endeavor™ DES(ゾタロリムス)(Medtronic Heart Valve Inc. USA),Resolute DES(ゾタロリムス)(Medtronic Heart Valve Inc. USA),Nobori®DES(バイオリムス)(Terumo Corporation, Japan)が入手可能だが,いずれも冠動脈が適応であり,肺静脈への使用はoff-label useとなる.
また左心低形成症候群およびそのvariantに対する1st.stageとしてのhybrid治療においては,専用の動脈管用stentとしてself-expandingのsinus-SuperFlex-DS stent(OptiMed, Germany)(Fig. 4-G)が市場化されている.径は4~9 mm,長さは径によって12または15から24 mmで,いずれも4Frシースに適合する.またCoA合併症例に対してはCoA部分に専用のsinus-Repo-DS stent(OptiMed, Germany)(Fig. 4-H)が用いられるが,いずれも国内には未導入である.
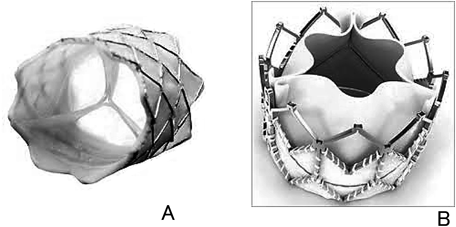
肺動脈弁に関しては,狭窄に対しては経皮的バルーン弁形成術が選択肢だが,効果は一定でなくかつ逆流増加のデメリットも併存する.これを解決し,かつ逆流に対しても効果を発揮するのが経皮的肺動脈弁留置術である24).Melody® Transcatheter Pulmonary Valve(Fig. 5-A)は右室流出路の弁機能不全に対してデザインされた人工弁で,グルタール処理されたウシ静脈弁を,platinum iridium合金のstent内に縫着したものである.ウシ静脈弁は低圧でも良好に開放・閉鎖し,かつ弁尖のcoaptationが深いため,広範囲の直径に対応してその形態を維持できる.ウシ静脈弁の径が16 mmのものでは20 mmまで,18 mmものは22 mmまで拡大できる.これを,Balloon-in-balloon(BIB)上にマウントして留置する.BIBを用いることで,拡大中に弁が最適な位置に留置できるよう調整がしやすくなる.さらに,三尖弁位への経皮的留置や25),特に体格の小さい乳児において僧帽弁位へのhybrid法を用いた留置にも用いられるなど26)使用範囲が拡大している.Edwards SAPIEN® Transcatheter Heart Valveは成人の大動弁位への留置を目的として開発されたが,肺動脈弁位へその適応が拡大し,欧米ではEdwards SAPIEN XT® Transcatheter Heart Valve(Fig. 5-B)が肺動脈弁位の適応となっている.石灰化を低減するCarpentier-Edwards ThermaFix Tissue Processという手法を用いて処理したウシ心膜で三尖弁を形成し,cobalt chromium合金のstentに縫着したものである.径23 mm, 26 mm, 29 mmの3種類あり,20~29 mmの右室流出路径に対応している27).すなわちMelody® Transcatheter Pulmonary Valveより径の大きい症例にも挿入可能である.国内には上記いずれのvalveも導入されていない.
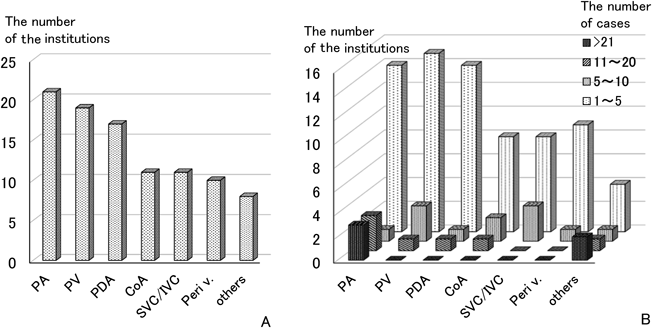
以上のように,日本ではdeviceの導入が遅い上に,先天性心疾患への適応がないdeviceが非常に多いことから,適応に準じた使用のみに頼っていたのでは治療の幅が極めて狭くなることが明らかである.したがって我々はoff-label useを選択せざるを得ない状況下に置かれているのであるが,実際にはどのようなoff-label useがどのくらいの頻度で施行されているのであろうか.第27回JPIC学術集会(於:広島国際会議場,会長:鎌田政博)ではこの問題を主要テーマの一つとして取り上げアンケート調査を行った.off-label useはある意味“公然の秘密”とも呼べる使用法であり,実情をすべて把握するのが困難であることは想像に難くない.この調査は敢えてその領域に踏み込み,off-label useの問題に対する“breakthrough”として重要な意味をもつものと考えられる.対象は日本小児循環器学会修練施設の133施設,および日本心血管インターベンション治療学会(CVIT: Japanese Association of Cardiovascular Intervention and Therapeutics)所属の27施設で,各施設にe-mailまたは郵送でoff-label useとdevice lagに関する質問票を配布し,専用web siteでのon line入力で回答を収集した.質問票を送付した160施設のうち39施設(小児循環器学会修練施設33施設,CVIT関連6施設)から回答を得た(回収率24%).Off-label useの経験がある施設は29施設(74%)に上り,off-label useがもはやある意味一般化していることが示唆された.stentが最も多くの施設でoff-label useの経験があり25施設,続いてAVPが11施設,ASOが10施設,ADOが7施設,その他のdeviceが3施設であった.Stentでは,使用の対象病変部位は肺動脈が最も多く(21施設),肺静脈(19施設),動脈管(17施設),大動脈縮窄(11施設),大静脈(11施設),末梢血管・静脈(10施設),その他(8施設)であった(Fig. 6-A).使用症例数に関しては肺動脈への使用が21例以上に上る施設が3施設,11~20例の施設が3施設と,他の疾患に比較してもかなり肺動脈へのstent off-label useが行われていることがうかがわれた(Fig. 6-B).
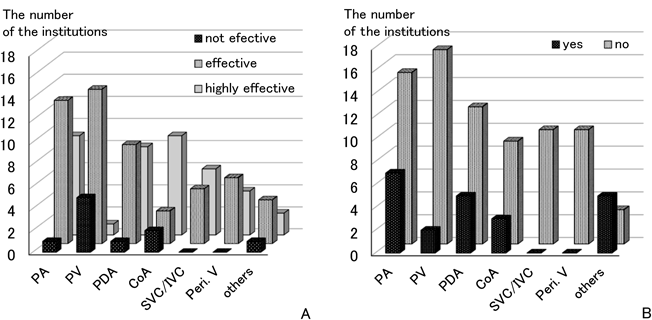
stentのoff-label useの効果に関しては著効,有効が圧倒的に多かったが,肺静脈に関しては無効との回答が使用した20施設中5施設で見られた(Fig. 7-A).ただしこれには原疾患の質が大きく関与しているであろうことは,これまでの報告からも容易に推測され23),stentのoff-label useを否定的に捉える根拠とはならないものと考えられる.重篤な有害事象(死亡,外科治療など侵襲的な治療を必要とする,あるいは永続的な障害が残ったもの)に関しては,大静脈,末梢血管へ施行した施設ではその経験がなかったが,肺動脈,肺静脈,動脈管,大動脈縮窄では11~32%の施設でその経験があった(Fig. 7-B).ただしこれは過去に一例でも有害事象を経験したことのある施設の数を集計した結果であって,有害事象を認めた症例数を示すものではない.しかしながら“適応外”という性質上,見過ごせない数字である.
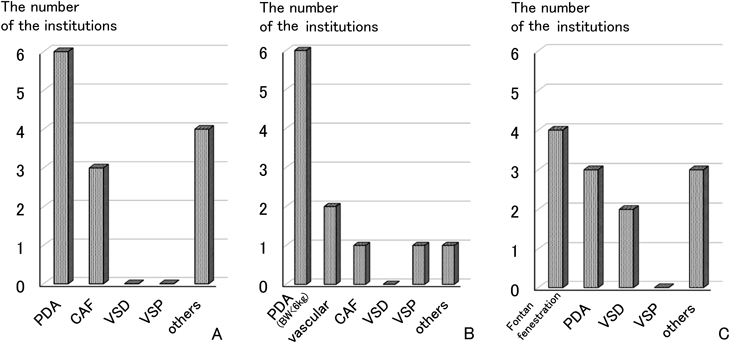
そのほかのdeviceでは,AVP, ADOとも動脈管へのoff-label use経験を有する施設が最も多く,冠動脈瘻がこれに続いていた(Fig. 8-A, B).ASOではFontanの開窓が最も多く,動脈管,心室中隔欠損への使用も見られた(Fig. 8-C).
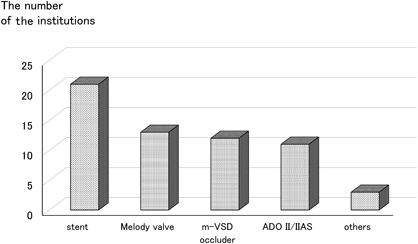
早期の導入が望まれるdeviceとしてはstentを挙げる声が最も多く,Melody® Transcatheter Pulmonary Valve, muscular VSD device, ADOII/IIASが続いていた(Fig. 9).AVP, ADOとも前述のとおり動脈管へのoff-label useが多く,これにはADOの適応が体重>6 kgであることが関与していることは容易に推測され,ADOII/IIASの導入が望まれる背景となっていると考えられる.
わが国の先天性心疾患に対するカテーテル治療のレベルを周辺諸外国と比較してどう感じるか,という質問に関しては,アジア諸国に比較しても63%が,欧米諸国のとの比較では82%と非常に多くの施設が遅れを感じていた.
最後に,自由記載のコメントには,
- ・海外で手技の安全性および必要性が担保されているdeviceに関しては,早期導入,Off-label useの容認
- ・臓器特異的な保険適応の廃止
- ・希少使用における治験などの簡略化や負担軽減など,企業にインセンティブを与える方策の確立
などの提案が見られた.
各種deviceのoff-label useは先天性心疾患領域のみの問題ではなく,かつ国内のみの問題でもない.例えばTAXUS® drug eluting stentの使用に関しては,その約65%がoff-label useであったとの調査結果が出ている28).またTable 1の承認状況,承認年度を見ても明らかなように,CEに比較してFDAで認可を得る方が基準が厳しく,一般に長い調査期間を要している.このためUSAにおいても先天性心疾患領域では非常に多くのdeviceをoff-label useに頼っているのが現状で,Sutherellらの3年間の経験では,先天性心疾患のカテーテル治療に使用されたdeviceのうち63%がoff-label useで,特にstentでは99%がoff- label useであった29).これにはUSAでもCP Stent™,Covered CP Stent™が大動脈縮窄症に対して認可(2016年3月)されるまで,先天性心疾患に認可されているstentは一つとして存在しなかったという背景が関連している.
何がon-label useまでの道を困難なものにしているのであろうか.一つには我々の治療対象が多種多様にわたり,かつそれぞれがlow volumeであることが挙げられる29, 30).血管形成術を例に挙げると,治療対象血管として主肺動脈,肺動脈枝,大動脈およびその分枝,動脈管,短絡血管(人工血管を含む),大静脈(人工血管を含む),肺静脈など多岐にわたる.これに対して現状では冠動脈stent,末梢血管stent,腸骨・腎動脈stent,胆管stentなど様々なstentを用いている.加えてstentの新規開発,導入のサイクルは比較的早い.つまり,もともとの対象数が少ないうえに治療選択肢は多く,かつそれが短期間で入れ替わるという現象が起き,それぞれにおいて十分な検討に至るまでの症例数は集積しないというのが実情である30).
また,胆管stentを例に挙げると,FDAで認可を取るために必要なデータは,血管への使用に比較して血管外使用のほうが決定的に少なくて済む.したがって血管への使用で適応を取る代わりに血管外使用で適応を取ることは非常に安上がりな「裏口」になる.これは決して望ましい状況ではないが,胆管で認可を得たstentの血管内使用はもはや当然のように行われ,先天性心疾患に関連する血管内治療の主軸にさえなっている30).そして国内ではFDAの認可があることを基礎に認可申請を行っていくことが多いため,FDAが上記のような状態では,国内での認可対象が血管に拡大されることは,ほぼ期待できない.
このように実際には非常に多数のoff-label useが行われることになっていくわけだが,明らかな適応上の警告を無視するのは安易なことではない.off-label useでは万が一合併症が発生した際にはそれを施行した臨床医が法的に守られることは非常に難しく,法律家の目から見れば薄氷の上に立っているようなものだと評される31).そして臨床家たちも十分そのことは承知している.今回のアンケート調査でも,肺動脈,肺静脈,動脈管,大動脈縮窄の治療においては11~32%の施設で重篤な有害事象の経験があり,看過できない数字である.またアンケートの回答率も29%と高い数字ではなかった.ここには回答を躊躇する上記のような背景が影響している可能性も考えられる.
しかしながら,適応上の制限や警告は現実に即したものでないことも多く,そのdeviceの使用こそが病変部の問題解決に最適の方法であると考えられる場面に,臨床家であればほぼ誰もが遭遇する30).そして自分たちの危うい立場を十分承知のうえでも,off-label useが最善の手段という判断を下し,施行している.もちろんその際にはOff-label useによる有害事象の可能性も十分考慮に入れているはずである.有害事象は何もoff-label useのみで発生するのもではない.他の認可されている治療法で病変部の問題が十分解決できるのか,それによる有害事象もしくは治療侵襲の大きさはどうかなどを検討したうえで臨床家はoff-label useの決断を下している.これが実情ではなかろうか.Off-label useに対する批判には,臨床医がこれだけ十分注意深く検討したうえでの決定だという点が看過されている向きがあるように思われる30).
この問題解決には,臨床家から国の認可機関への積極的な働きかけが必要になってくる.USAでも,小児に対してoff-label useされているdeviceに関して,適応拡大へ向けた調査が必要だとの認識から,2007年に,Pediatric Medical Device Improvement and Safety Act(PL-110-85)が設立された32).この法制定は小児に使用されているdeviceの市販後安全性調査を徹底する必要性を強調し,小児適応のdeviceの発展,開発を促進するための非営利組織を作ることを推奨している.これにより小児,および先天性心疾患に特有の病変に特化したdeviceの発展を促進させる助けになることが期待されている32).
我が国には以下のような機関が存在する.まず一つ目は,厚生労働省所管の法人である,独立行政法人医薬品医療機器総合機構(PMDA; Pharmaceuticals and Medical Devices Agency)である.これは独立行政法人医薬品医療機器総合機構法に基づいて,国立医薬品食品衛生研究所医薬品医療機器審査センター,医薬品副作用被害救済・研究振興調査機構および財団法人医療機器センターの一部の業務を統合し平成16年4月1日に設立された法人である33).PMDAは①医薬品の副作用や生物由来製品を介した感染等による健康被害に対して,迅速な救済を図ること(健康被害救済)②医薬品や医療機器などの品質,有効性および安全性について,治験前から承認までを一貫した体制で指導・審査すること(承認審査)③市販後における安全性に関する情報の収集,分析,提供を行う(安全対策)が主な業務となる.
二つ目は,厚生労働省の「医政局経済課医療機器政策室」である34).厚生労働省の「医療上必要性が高いにもかかわらず,我が国において未承認又は適応外の医療機器および体外診断用医薬品(以下「未承認医療機器等」という.)については,我が国に早急に導入されるべきである」という方針に基づき,平成18年よりこの医政局経済課医療機器政策室が「医療ニーズの高い医療機器等の早期導入に関する検討会」を開催し,学会などからの要望を踏まえて医療上必要性の高い未承認医療機器等の早期承認に向け動いている.
検討対象としては,
- (1) 未承認医療機器および体外診断用医薬品
- 要望の対象となる医療機器等は,原則として主要諸外国にて承認されているものであって,医療上特に必要性が高いと認められるものであること.
- (2) 適応外医療機器および体外診断用医薬品
- 要望の対象となる使用目的は,主要諸外国にて承認されている範囲であって,医療上特にその必要性が高いと認められるものであること.
と定められている.このうち,「医療上特に必要性が高いと認められるもの」は,[1]適応疾病の重篤性と[2]医療上の有用性の観点から総合的に評価され,[1]適応疾病の重篤性は,ア:生命に重大な影響がある疾患(致死的な疾患)であること,イ:病気の進行が不可逆的で,日常生活に著しい影響を及ぼす疾患であること,ウ:その他,である.[2]医療上の有用性は,ア:既存の治療法,予防法もしくは診断法がないこと,イ:欧米において承認されており,有効性,安全性,肉体的・精神的な患者負担の観点から,医療上の有用性が既存の治療法,予防法もしくは診断法よりすぐれていること,ウ:その他,となっている.最近では平成27年5月にこの検討会が行われたが,今後の運用等について見直しを行っているところとなっている34).
これらの機関に対し,我々臨床家が,先天性心疾患の患者がおかれている現状を報告し,device治療の可能性を訴え,働きかけていくことが,今後の導入,認可への糸口となるものと考えられる.
Balloon angioplasty中の血管破裂では,covered stentをバックアップしておき,発生時には速やかに挿入するという方法が欧米では常識となっている.しかし日本ではこの方法はこれまで現実的でなかった.技術的には遅れていないと自負したところで,device lagのために一歩国外に出ると同じ土俵に立って会話をすることさえできないという現状がある.この現状に我々各人が問題意識をもって臨み,今こそアクションを起こしていくことが必要であろう.
最後に第27回JPIC学術集会のアンケート調査にご協力いただいた施設の先生方に感謝申し上げます.
引用文献References
1) 富田 英:先天性心疾患に対するカテーテル治療 ~本邦への導入が期待されるdevice~.日本小児循環器学会雑誌2012; 28: 168–173
2) Javois AJ, Rome JJ, Jones TH, et al: Gore HELEX Continued Access Study Group: Results of the U.S. Food and Drug Administration continued access clinical trial of the GORE HELEX septal occluder for secundum atrial septal defect. JACC Cardiovasc Interv 2014; 7: 905–912
3) Spencer FA, Lopes LC, Kennedy SA, et al: Systematic review of percutaneous closure versus medical therapy in patients with cryptogenic stroke and patent foramen ovale. BMJ Open 2014; 4: e004282. DOI: 10.1136/bmjopen-2013-004282
4) Li J, Liu J, Liu M, et al: Closure versus medical therapy for preventing recurrent stroke in patients with patent foramen ovale and a history of cryptogenic stroke or transient ischemic attack. Cochrane Database Syst Rev 2015; 8: CD009938. DOI: 10.1002/14651858.CD009938.pub2
5) Liddy S, Oslizlok P, Walsh KP: Comparison of the results of transcatheter closure of patent ductus arteriosus with newer Amplatzer devices. Catheter Cardiovasc Interv 2013; 82: 253–259.
6) Sungur M, Karakurt C, Ozbarlas N, et al: Closure of patent ductus arteriosus in children, small infants, and premature babies with Amplatzer duct occluder II additional sizes: Multicenter study. Catheter Cardiovasc Interv 2013; 82: 245–252. DOI: 10.1002/ccd.24905
7) Garay FJ, Aguirre D, Cárdenas L, et al: Use of the Amplatzer vascular plug II device to occlude different types of patent ductus arteriosus in pediatric patients. J Interv Cardiol 2015; 28: 198–204. DOI: 10.1111/joic.12188
8) Cubeddu RJ, Babin I, Inglessis I: The off-label use of the Amplatzer muscular VSD occluder for large patent ductus arteriosus: A case report and review. Cardiovasc Interv Ther 2014; 29: 256–260. DOI: 10.1007/s12928-013-0223-7
9) Alwi M: PDA occlusion with the Amplatzer devices, in Sievert H (ed): Percutaneous interventions for congenital heart disease. London, Informa Healthcare, 2007, pp. 377–384
10) Baspinar O, Irdem A, Kilinc M: Off-label use of Amplatzer devices in congenital heart disorders during childhood. Acta Cardiol 2013; 68: 31–35
11) Qureshi SA: Transcatheter closure of coronary artery fistulas, in Sievert H (ed): Percutaneous interventions for congenital heart disease. London, Informa Healthcare, 2007, pp. 421–430
12) Fu YC, Bass J, Amin Z, et al: Transcatheter closure of perimembranous ventricular septal defects using the new Amplatzer membranous VSD occluder: Result of the U.S. phase I trial. J Am Coll Cardiol 2006; 47: 319–325
13) Tzikas A, Ibrahim R, Velasco-Sanchez D, et al: Transcatheter closure of perimembranous ventricular septal defect with the Amplatzer membranous VSD occluder 2: Initial world experience and one-year follow-up. Catheter Cardiovasc Interv 2014; 83: 571–580. DOI: 10.1002/ccd.25004
14) Kang SL, Tometzki A, Caputo M, et al: Longer-term outcome of perventricular device closure of muscular ventricular septal defects in children. Catheter Cardiovasc Interv 2015; 85: 998–1005
15) Feltes TF, Bacha E, Beekman RH 3rd, et al: American Heart Association Congenital Cardiac Defects Committee of the Council on Cardiovascular Disease in the Young; Council on Clinical Cardiology; Council on Cardiovascular Radiology and Intervention; American Heart Association: Indications for cardiac catheterization and intervention in pediatric cardiac disease: A scientific statement from the american heart association endorsed by the american academy of pediatrics and society for cardiovascular angiography and intervention. Circulation 2011; 123: 2607–2652. DOI: 10.1161/CIR.0b013e31821b1f10
16) Al-Hay AA, Shaban LA, Al-Qbandi MA, et al: Occlusion of Fontan fenestration using Amplatzer septal occluder. Int J Cardiovasc Imaging 2011; 27: 483–490
17) Jeong SI, Huh J, Lee HJ, et al: Closure of conduit fenestration after extracardiac Fontan procedure using Amplatzer Vascular Plug: Comparison with detachable coil. Pediatr Cardiol 2010; 31: 44–49
18) Meadows J, Minahan M, McElhinney DB, et al: COAST Investigators: Intermediate outcomes in the prospective, multicenter Coarctation of the Aorta Stent Trial (COAST). Circulation 2015; 131: 1656–1664. DOI: 10.1161/CIRCULATIONAHA.114.013937
19) Taggart NW, Minahan M, Cabalka AK, et al: COAST II Investigators: Investigators immediate outcomes of covered stent placement for treatment or prevention of aortic wall injury associated with Coarctation of the Aorta (COAST II). JACC Cardiovasc Interv 2016; 14: 484–493. DOI: 10.1016/j.jcin.2015.11.038
20) Qureshi SA: Stenting in aortic coarctation and transverse arch/isthmus hypoplasia, in Sievert H (ed): Percutaneous interventions for congenital heart disease. London, Informa Healthcare, 2007, pp. 475–485
21) Wilson N: Relief of right ventricular outflow tract obstruction, in Sievert H (ed): Percutaneous interventions for congenital heart disease. London, Informa Healthcare, 2007, pp. 439–445
22) Laston L: Pulmonary artery stenosis, in Sievert H (ed) : Percutaneous interventions for congenital heart disease. London, Informa Healthcare, 2007, pp. 447–454
23) Balasubramanian S, Marshall AC, Gauvreau K, et al: Outcomes after stent implantation for the treatment of congenital and postoperative pulmonary vein stenosis in children. Circ Cardiovasc Interv 2012; 5: 109–117
24) Cheatham JP, Hellenbrand WE, Zahn EM, et al: Clinical and hemodynamic outcomes up to 7 years after transcatheter pulmonary valve replacement in the US melody valve investigational device exemption trial. Circulation 2015; 131: 1960–1970
25) Roberts PA, Boudjemline Y, Cheatham JP, et al: Percutaneous tricuspid valve replacement in congenital and acquired heart disease. J Am Coll Cardiol 2011; 58: 117–122. DOI: 10.1016/j.jacc.2011.01.044
26) Quinonez LG, Breibart R, Tworetsky W, et al: Stented bovine jugular vein graft (Melody valve) for surgical mitral valve replacement in infants and children. J Thorac Cardiovasc Surg 2014; 148: 1443–1449
27) Wilson WM, Benson LN, Osten MD, et al: Transcatheter pulmonary valve replacement with the Edwards Sapien System: The Toronto Experience. JACC Cardiovasc Interv 2015; 8: 1819–1827
28) Russell ME, Friedman MI, Mascioli SR, et al: Off-label use: An industry perspective on expanding use beyond approved indications. J Interv Cardiol 2006; 19: 432–438
29) Sutherell JS, Hirsch R, Beekman RH 3rd: Pediatric interventional cardiology in the United States is dependent on the off-label use of medical devices. Congenit Heart Dis 2010; 5: 2–7. DOI: 10.1111/j.1747-0803.2009.00364.x
30) Holzer R, Hijazi Z: The off-versus on-label use of medical devices in interventional cardiovascular medicine?: Clarifying the ambiguity between regulatory labeling and clinical decision making, Part III: Structural heart disease interventions. Catheter Cardiovasc Interv 2008; 72: 848–852
31) David Y, Hyman WA: Issues associated with off label use of medical devices. Conf Proc IEEE Eng Med Biol Soc 2007; 2007: 3556–3558
32) Bleicher EW: Encouraging research and development of pediatric medical devices through legislative and regulatory action: The Pediatric Medical Device Safety and Improvement Act of 2007 in context. Food Drug Law J 2009; 64: 531–564
33) 独立行政法人 医薬品医療機器総合機構ホームページ:https://www.pmda.go.jp/about-pmda/outline/0001.html
34) 厚生労働省 ホームページ:医療ニーズの高い未承認医療機器等の早期導入に関する要望の募集について.http://www.mhlw.go.jp/stf/seisakunitsuite/bunya/kenkou_iryou/iryou/soukidounyuu2/