静脈血栓塞栓症に対するカテーテル治療に関して,本邦では肺血栓塞栓症に対してのガイドラインがあるが,血栓吸引の際,デバイスの選択は施設や術者ごとで異なる.複数の経皮的血栓除去用カテーテルが開発されているものの,そのすべてを施設内にそろえておくことは困難で,施設内にあるデバイスを駆使して血栓溶解,血栓吸引術を行う必要がある.今回,Fontan術後遠隔期に深部静脈血栓を来し,血栓吸引の際にアブレーション用の8.5 French(Fr)可変式シースが有用であった症例を経験したため,ここに報告する.
22歳女性.主訴は左頸部・腋窩・前腕の疼痛,左上肢腫脹.
現病歴はEbstein病,Fontan術後で当科にて追跡中,受診4日前に起床時より左頸部・腋窩・前腕の疼痛,左上肢の腫脹を認め,左上肢の腫脹が増悪したため当科を受診した.
既往歴:1歳1カ月時に左Blalock–Taussigシャント,1歳2カ月時にStarns手術,心房中隔作成術,右房縫縮術,1歳4カ月時に完全房室ブロックのためにペースメーカ移植術,2歳10カ月時に両方向性Glenn手術,4歳11カ月時心外導管を用いたFontan手術を施行.10歳時に蛋白漏出性胃腸症発症,11歳右横隔膜縫縮術,19歳時に原発性無月経のためホルモン補充療法開始.19歳時の心臓カテーテル検査では肺動脈平均圧10 mmHg,左室収縮期圧87 mmHg,拡張末期圧10 mmHg,左室拡張末期容積70% of normal,左室収縮率56%,心係数2.1 L/min/m2.
家族歴は特記すべきことなし.飲酒,喫煙歴はなし.
内服:フロセミド(80 mg/day),スピロノラクトン(50 mg/day),トルバプタン(7.5 mg/day),アスピリン(100 mg/day),ロキサチジン(37.5 mg/day),Lアスパラギン酸カルシウム(1800 mg/day),エストラジオール(0.72 mg 2日に1回張り替え),クロルマジノン酢酸エステル(4 mg/day),エルデカルシトール(0.5 µg/day)
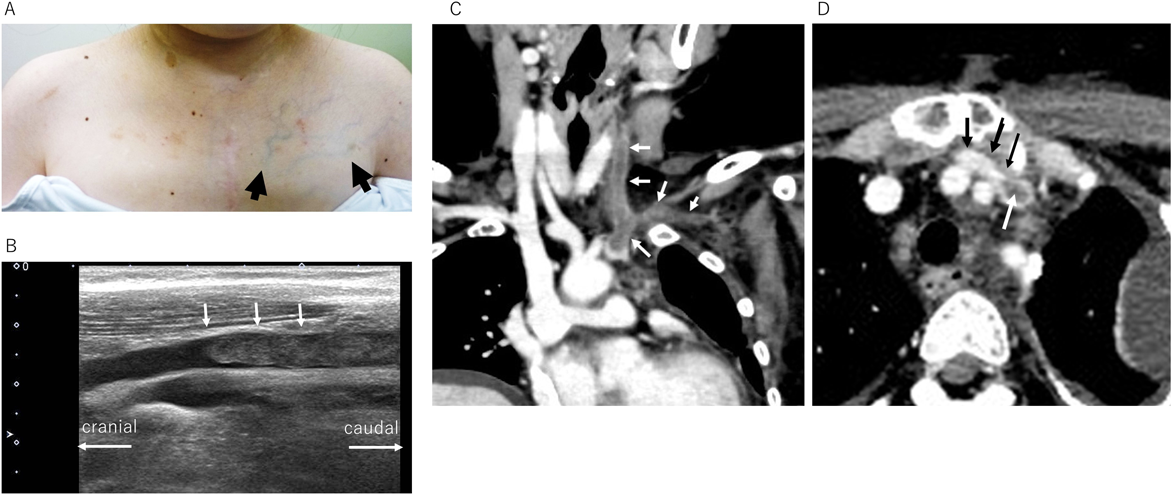
来院時現症:身長147 cm,体重44.8 kg,体温36.2°C,心拍数93回/分,血圧108/39 mmHg,呼吸数28回/分,酸素飽和度96%,意識声明,左頸部から腋窩,前腕にかけて疼痛あり,左前胸部の表在静脈怒張(Fig. 1A),左上肢の発赤,腫脹あり,心音整,心雑音は聴取せず.腹部はやや膨満,肝臓は左季肋部に2 cm触知.
WBC 6800/µL, RBC 3.89*106/µL, Hb 7.9 g/dL, PLT 72.2*103/µL, PT 105%,PTINR 0.98, APTT 25 s, D-dimer 2.75 µg/L(−0.85),CRP 0.09 mg/dL, TP 3.9 g/dL, Alb 1.8 g/dL, AST 24 IU/L, AST 22 IU/L, LDH 174 IU/L, γGTP 28 IU/L, BUN 11.3 mg/dL, Cre 0.56 mg/dL, Ca 7.1 mg/dL, Na 137 mmol/L, K 3.9 mmol/L, Cl 108 mmol/L, Tcho 131 mg/dL, TG 133 mg/dL, Tbil 0.2 mg/dL, CK 103 U/L, UA 2.7 mg/dL PCT-Q 0.13 ng/mL, BNP 18.4 pg/mL
AT 128%(正常値80–130%),プロテインC活性128%(80–120%),プロテインS活性102%(56–126%),ループスアンチコアグラント0.72(1.2以下),抗核抗体陰性,抗カルジオリピンβ2GPI複合体抗体1.3 U/min(3.5 U/min未満),C3 141.7 mg/dL(69–128),C4 27.2 mg/dL(13.6–36)
胸部レントゲン:心胸郭比53%,左上肺野に異常陰影あり(胸水を示唆する).
心電図:洞調律87 bpm, PR 231 ms, 完全石脚ブロック, QRS幅129 ms, Pacemakerは心房,心室ともにセンシング.
心エコー:LVDd 42 mm, LVDs 29 mm, LVEF 59%,右SVC内に血栓を認めず.
超音波:左内頸静脈から左鎖骨下静脈にかけて血栓を認める.エコー輝度は不均一でやや高輝度.石灰化はない.左内頸静脈は完全閉塞(Fig. 1B).
造影CT:左内頸静脈,鎖骨下静脈,無名静脈内に血栓を認め,無名静脈の血栓は幅9 mm,長さ7.5 cm.無名静脈は血栓の近位部(右側)で前方は胸骨,後方は総頸動脈,左内頸動脈で挟まれている.右横隔膜挙上,少量の腹水を認めた(Fig. 1C, D).
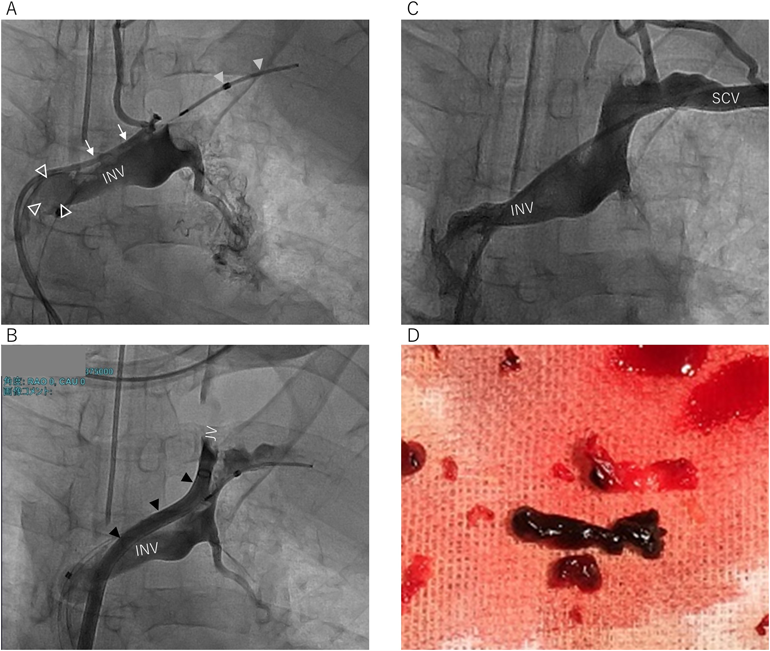
入院当日に緊急で血栓吸引術を施行した.全身麻酔下で右大腿静脈に5 Frシース,左大腿静脈に6 Frシース1本,7 Frシース1本を挿入.それぞれから血栓溶解カテーテル(FOUNTAIN® Infusion catheter, 4 Fr, 90 cm, Infusion部5 cm, Merit Medical Systems Inc., South Jordan, UT, USA),ニプロオクルージョンカテーテル(4 Fr, balloon 20 mm, Nipro Occlusion Catheter, Nipro, Osaka, Japan),吸引カテーテル(Eliminate®+, 7 Fr, XL, Terumo, Aichi, Japan)を挿入した.血栓が肺動脈に飛散するのを防ぐため,ニプロオクルージョンカテーテルを無名静脈基部で膨らませ,ウロキナーゼ(12万単位)をFOUNTAIN® Infusion catheterから血栓部位に散布しながら,Eliminate®+(7 Fr, XL)で吸引を行った(Fig. 2A).しかし血栓を吸引できなかったため,Agilis™ NxT Steerable Introducer(8.5 Fr, Abbott Inc, St. Paul, MN)に変更した.容易に血栓の吸引が可能となり,残りのウロキナーゼ(12万単位)を散布しながら,血栓吸引を繰り返した(Figs. 2B, C, D).先端がソフトチップであること,可変であることからシースのみで鎖骨下静脈,内頸静脈にすすめ,シース先端を血栓に押し付けながらシースのサイドポートの三方活栓から血栓吸引を行った.その後の造影で左肺動脈下葉枝の一部に造影不良領域を認め,血栓の飛散を疑った.出血量は300 mL,赤血球輸血を420 mL行った.抜管ののちICU入室.翌日一般病棟に退室.APTT 60秒を目標にヘパリン持続投与を開始し,ワーファリンに置換した.ウロキナーゼの持続投与(入院初日から4日目までは18万単位/day, 5日目から9日目までは12万単位/day)を併用した.3週間後に心臓カテーテル検査,造影検査を施行.左肺動脈を含め血栓を認めず.左肺動脈平均圧 11 mmHg,右肺動脈平均圧 17 mmHg,上大静脈 17 mmHg,下大静脈 13 mmHg,左室収縮期圧 114 mmHg,拡張期末期圧 5 mmHg,左室収縮率 56%,心係数は3.4 L/min/m2であった.第24病日に退院となった.病理検査では吸引した血栓は数日以内に生じたとの結果であった(血球成分とフィブリンが混在,ヘモジデリンは伴わない.血栓外側に線維芽細胞を認める).
フォンタン手術後の深部静脈血栓症(左内頸,鎖骨下静脈)に対して内腔8.5 Frの可変シース(Agilis)を用いて効果的に血栓吸引が可能であった1例を経験した.
フォンタン手術後の血栓症
フォンタン手術後の血栓症は17–33%に発症すると報告されている1–3).そのリスクファクターとして導管狭窄,高い静脈圧,蛋白漏出性胃腸症,心房性不整脈,凝固因子の異常,肺動脈スタンプなどがある4, 5).本症例では低心拍出,蛋白漏出性胃腸症の存在,ホルモン補充療法,無名静脈の狭窄,多剤の利尿剤内服が血栓の発生と関連していたと考えられた.これ以上のフォンタン循環の改善は難しいため,血栓吸引後はホルモン補充療法の中止,ワーファリン追加を行った.
血栓に対する治療
日本循環器学会のガイドラインには発症早期で血行動態が不安定な肺塞栓症,症状が強い腸骨大腿静脈血栓症に対してカテーテル治療が有効であるとの記載がある6).一方フォンタン手術後の血栓症はしばしば認められ抗凝固療法が行われるのが一般的である.血行動態が不安定な肺動脈血栓,中心性深部静脈血栓に対して少数であるがカテーテル治療が行われている7–9).今回入院日に緊急でカテーテルでの血栓吸引を行った.血栓形成から数日以内,肺動脈への血栓が飛ぶこと,既に左胸水貯留が見られておりフォンタン循環の破綻が危惧されたこと,解剖学的に無名静脈が狭いことから薬物治療の効果が限定的であると判断してカテーテル治療を選択した.
カテーテル血栓溶解療法と血栓除去術
カテーテル治療には血栓溶解療法と血栓除去術がある.血栓溶解療法はカテーテルからウロキナーゼ24万単位やtPA製剤13750単位/kgを投与する.血栓吸引療法は海外ではAngioJet™10)やAngioVAC7)が使用できるが,日本ではピッグテイルカテーテルを回転させながら血栓を破砕したり,血栓吸引カテーテルやガイディングカテーテル(Thrombobuster(Kaneka Medics, Tokyo, Japan),Heartrail®(Terumo, Tokyo, Japan),Launcher™(Medtronic, Minneapolis, MN))を用いた報告がある8, 9).
今回以下の2種類のカテーテルを用いて血栓溶解・吸引を試みた.FOUNTAIN® Infusion catheterは多孔性の血栓溶解カテーテルであり,eliminate®+は遠位の内腔の径が1.3 mmの血栓吸引カテーテルである.しかし9 mm大の血栓に対して効果はなかった.そのためAgilisを使用した.ウロキナーゼを投与予定量の半量の12万単位使用した時点で血栓が溶解する印象はなく,血栓形成から4–5日経過していたことがその原因と考えられる.フォンタン術後の血栓は太い静脈系(肺動脈も含めた)に起こることがほとんどであり細いカテーテルで吸引は難しい.太いカテーテルでしっかり血栓に押し付けながら吸引することで容易に吸引できた.
今回用いたAgilisは先端が柔らかく,内腔が大きい可変シースで大きな血栓を吸引でき,シースだけで目標血管に安全に到達できる点で有用であり,通常の方法で血栓吸引が困難な場合の選択肢になり得る.
フォンタン手術後の深部静脈血栓症(左内頸,鎖骨下静脈)に対して内腔8.5 Frの可変シース(Agilis)を用いて効果的に血栓吸引が可能であった1例を経験した.通常の方法で血栓吸引が困難な場合に有用な選択肢になり得る.
引用文献References
1) Monagle P, Cochrane A, McCrindle B, et al: Thromboembolic complications after fontan procedures—the role of prophylactic anticoagulation. J Thorac Cardiovasc Surg 1998; 115: 493–498
2) Balling G, Vogt M, Kaemmerer H, et al: Intracardiac thrombus formation after the Fontan operation. J Thorac Cardiovasc Surg 2000; 119: 745–752
3) McCrindle BW, Manlhiot C, Cochrane A, et al: Fontan Anticoagulation Study Group: Factors associated with thrombotic complications after the Fontan procedure: A secondary analysis of a multicenter, randomized trial of primary thromboprophylaxis for 2 years after the Fontan procedure. J Am Coll Cardiol 2013; 61: 346–353
4) Kaulitz R, Ziemer G, Rauch R, et al: Prophylaxis of thromboembolic complications after the Fontan operation(total cavopulmonary anastomosis). J Thorac Cardiovasc Surg 2005; 129: 569–575
5) Firdouse M, Agarwal A, Chan AK, et al: Thrombosis and thromboembolic complications in fontan patients: A literature review. Clin Appl Thromb Hemost 2014; 20: 484–492
6) 肺血栓塞栓症および深部静脈血栓症の診断,治療,予防に関するガイドライン(2017年改訂版).Circulaton Journal 2017
7) Al-Hakim R, Patel K, Moriarty JM: AngioVac aspiration for paradoxical emboli protection through a fenestrated Fontan during central venous thrombus manipulation. Cardiovasc Intervent Radiol 2015; 38: 752–754
8) Hirono K, Ibuki K, Tomita H: Percutaneous catheter aspiration thrombectomy for the occluded stents of pulmonary artery in children with single ventricle physiology after fontan surgery. Catheter Cardiovasc Interv 2014; 84: 1153–1156
9) Kodama H, Shiina Y, Kijima Y, et al: Percutaneous aspiration embolectomy is beneficial for pulmonary thromboembolism in adult patients with Fontan circulation. J Cardiol Cases 2022; 26: 101–103
10) Donnelly JP, Ryan TJ Jr: Revascularization of a thrombosed aortopulmonary shunt with the use of the AngioJet thrombectomy system. Catheter Cardiovasc Interv 2003; 58: 268–271